

NAD+ and NMN are sold as supplements and, in clinical settings, prepared as compounded medications. The human evidence that either slows aging is limited. What follows is about the quality of a decision, not a promise that either compound does what the label implies.
I have come to believe that most expensive mistakes are not dramatic. They are quiet, repeatable, and almost boring, which is exactly why they keep happening. Nobody sets out to buy a mislabeled vial off a research-chemical site. They arrive there by a series of small, reasonable-feeling steps: a certificate that looked official, a headline that promised too much, a checkout page that never mentioned a doctor. The NAD+ and NMN market has, over the past few years, become a kind of laboratory for this exact phenomenon. Watch enough buyers move through it and you start to see the same seven missteps recur, in the same order, for the same reasons, regardless of who is doing the buying.
So this piece is not a warning in the usual sense. It is closer to a field guide. I want to name the seven mistakes plainly, weigh what each one actually costs (in bodily risk and in wasted money, because those are different currencies and people confuse them), and then point at the specific structural feature that makes each mistake simply impossible to make. The goal is to stop asking “which brand feels trustworthy” and start asking “which setup removes the choice to be careless.”
Scoring the damage
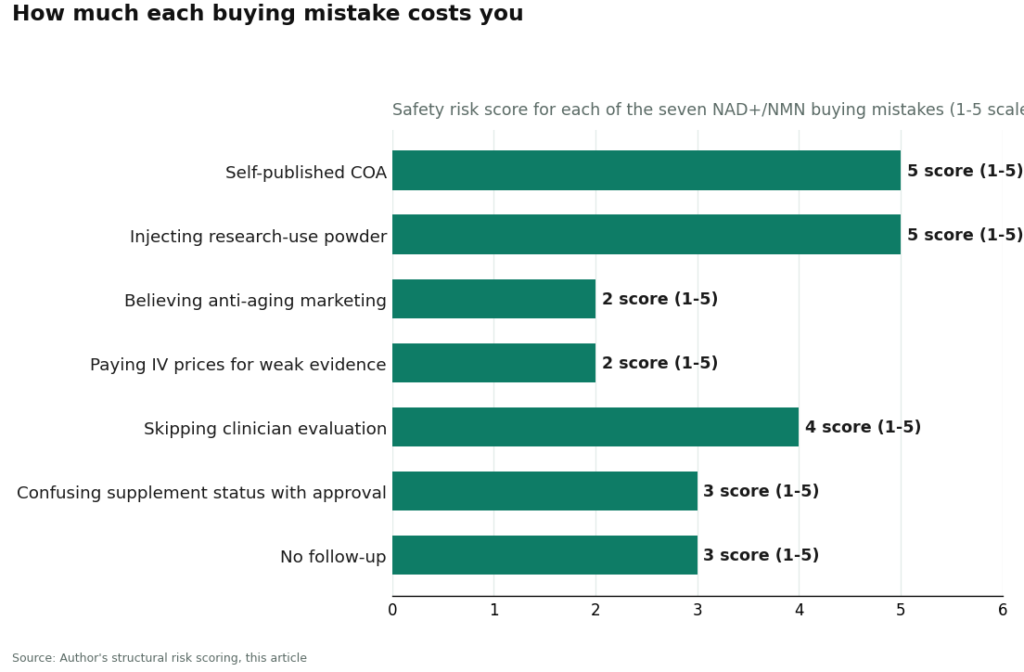
Here is the method, since a scorecard is only useful if you can see how it was built. Each mistake gets a Safety cost from 1 to 5 (5 meaning it could genuinely hurt you) and a Money cost from 1 to 5 (5 meaning you will reliably burn cash on nothing). The last column names the structural feature, not the vibe, that closes the gap.
| # | Mistake | Safety cost | Money cost | Structurally avoided by |
|---|---|---|---|---|
| 1 | Trusting a self-published certificate of analysis | 5 | 3 | Licensed pharmacy dispensing under named standards |
| 2 | Buying “research use only” powder to inject | 5 | 2 | A required clinician consult and prescription |
| 3 | Believing the anti-aging marketing | 2 | 5 | Honest, studied-not-proven framing |
| 4 | Paying premium IV prices for the weakest evidence | 2 | 5 | A clinician who weighs route against evidence |
| 5 | Skipping any clinician evaluation | 4 | 3 | Mandatory history review before dispensing |
| 6 | Confusing “sold as a supplement” with “approved” | 3 | 3 | A provider that states the real status |
| 7 | No follow-up, so problems go unmanaged | 3 | 2 | An ongoing clinician relationship |
Sit with that table for a minute and a pattern surfaces on its own. The three mistakes that could actually hurt you (1, 2, 5) are all closed by the same door: a licensed clinician and a licensed pharmacy standing between you and the vial. The two mistakes that hollow out your wallet (3, 4) are closed by something much cheaper than a pharmacy license: honesty about what the studies actually show. Oversight and honesty. That, it turns out, is the entire difference between a supervised medical provider and a research-chemical storefront with better photography.
Mistake 1: mistaking a document for a guarantee
The costliest mistake dresses itself up as diligence. A buyer finds a product page with a certificate of analysis attached, sees a lab name and a column of numbers, and relaxes. But a self-published COA is, structurally, just a document the seller chose to publish. It tells you that some sample, at some point, tested a certain way. It tells you nothing about whether the vial in your hand matches that sample, whether the lab was independent, or who answers for it if the two don’t match. For a seller with no license on the line, a COA is marketing wearing a lab coat. And with NMN in particular, a buyer has no real way to verify purity between competing brands on their own.
What closes this gap isn’t a better-looking certificate. It’s a licensed pharmacy, dispensing under recognized compounding standards, where an actual license, not a PDF, is on the hook for what leaves the building.
Mistake 2: the research-use label that isn’t a formality
This is the one with real teeth. Research-chemical NAD+ is inexpensive, and the “research use only, not for human consumption” phrase reads like fine print. It isn’t. It is the legal hinge that keeps the product outside drug regulation in the first place. Sell it for injection or ingestion and it becomes, in the eyes of the law, an unapproved drug, which is precisely why the label insists otherwise in writing.
Inject something with no clinician, no prescription, no dispensing pharmacy, and no check on identity, strength, or purity, and the quality control job has quietly become yours. If the vial is mislabeled or contaminated, nobody is coming to recall it. The fix here is not caution. It’s a required clinician consultation and prescription, meaning a licensed prescriber decided this was reasonable for you before it ever reached a vial.
Mistake 3: believing the story ahead of the data
The marketing on both compounds outruns the science by a wide margin, and believing it is what drains people’s wallets. So let me lay out the honest version, because it is the only real antidote.
NAD+ genuinely does decline with age, measured directly in human tissue in a 2012 study spanning newborn to age 77 [P5][5]. Precursors do something mechanically real: a 2018 placebo-controlled crossover trial of nicotinamide riboside, NMN’s close chemical cousin, was well tolerated and raised NAD+ in healthy middle-aged and older adults [P3][3]. NMN itself has a small handful of legitimate human trials. The strongest, a 2021 study in Science, gave 250 mg per day for 10 weeks to 25 prediabetic postmenopausal women and found improved muscle insulin sensitivity [P1][1]. A 2021 trial in amateur runners found some improved aerobic measures on NMN, though VO2max itself did not budge [P2][2].
None of that adds up to reversed aging. A 2026 PRISMA-guided systematic review found no eligible outcomes trials testing IV or IM NAD+ for anti-aging or wellness purposes at all, while confirming that oral precursors reliably raise NAD-related biomarkers, with human outcomes still mixed [P6][6]. The foundational review of NAD+ biology is blunter still: whether restoring NAD+ in aging humans is even safe long-term, let alone beneficial, remains unknown [P4][4]. What protects your money here isn’t skepticism for its own sake. It’s a provider willing to say “studied” instead of “proven.”
Mistake 4: paying the most for the least evidence
This is the mistake that should embarrass the market more than it does, because the pricing runs backward. IV NAD+ drips are sold as the premium tier, priced like serious medicine. But the controlled evidence for that exact route is close to nonexistent: the 2026 review found no eligible outcomes trials for IV or IM NAD+ whatsoever [P6]. Meanwhile the cheapest option on the shelf, an oral precursor, is the one that reliably moves NAD+ markers in the body [P3][P6]. You can, quite easily, pay the most for the route with the least to show for it.
None of this means a supervised IV drip is worthless. It means its value sits in oversight and sourcing, not in a proven biological effect, and the person who should be telling you that is a clinician weighing route against evidence, not an IV bar with a price list.
Mistake 5: no evaluation at all
Some sellers, and a surprising number of self-styled “clinics,” let anyone through with a thirty-second quiz that approves every answer. That is not an evaluation, it’s a formality with a checkbox. Skip a genuine review and nobody is checking whether either compound makes sense given your history, your medications, your conditions. For a compound this under-studied, especially one you might inject, that gap is a real safety problem, and it also wastes money on something that was never right for you to begin with. What closes it is a mandatory clinician review of your history before anything gets dispensed, and a prescription written only when it’s actually warranted.
Mistake 6: “sold as a supplement” is not “approved”
NMN’s regulatory status has shifted in a way that has confused almost everyone, and the confusion is costly. In 2022 the FDA said NMN was excluded from the supplement definition because it had already been authorized for investigation as a drug. After a citizen petition and litigation, the agency reversed itself: in letters dated September 29, 2025, it concluded NMN is not excluded from the dietary-supplement definition, citing evidence that NMN had been marketed as a supplement before that drug authorization [P7]. A December 2025 follow-up reportedly reinstated an earlier new-dietary-ingredient acknowledgment [P7].
The trap is reading “lawfully sold as a supplement” as “approved and proven.” It is neither of those things. NMN remains a new dietary ingredient subject to premarket notification, and supplement status has never been the same thing as drug approval. NAD+ by injection lives in the compounded category, also not an approved finished drug. What actually protects you is a provider willing to say the regulatory status plainly instead of letting the blur do the selling.
Mistake 7: treating the purchase as the finish line
The last mistake is quieter than the rest but no less real: assuming the transaction ends the relationship. With a compound whose effects remain uncertain, you want somewhere to report a side effect, ask a question, or adjust course. A research-chemical order ends at the shipping confirmation email. What closes this is simply an ongoing relationship with a clinician and an actual path to raise a problem.
Follow-up, though, only works if you bring something to it. Since the benefits of either compound are still uncertain, your own record over time is one of the few honest signals available to you. Logging dose, energy, and any symptoms, using something like the FormBlends tracker app, gives you something concrete to hand a clinician instead of a vague impression. It’s a logging tool. Nothing more, nothing for sale, no checkout attached to it.
Where the seven mistakes become structurally impossible
Score providers on the same axes, on whether their structure prevents these mistakes rather than merely promising to, and the field splits cleanly.
FormBlends comes out on top because its structure blocks every one of the seven. It is a supervised telehealth and compounding provider, not a supplement shelf and not a research-chemical warehouse. In its own public materials, NAD+ sits among its longevity compounds described in studied terms (“studied for cellular energy and metabolic support”), not sold as a cure for aging, with NMN in the same supervised, oral category. Access runs through a clinician: the site states plainly that all compounded medications require a licensed physician consultation and prescription, and that everything is prepared by licensed 503A compounding pharmacies following USP <797> and <800> standards.
Lay that against the scorecard and the fit is exact. The self-published-COA mistake (1) is blocked by licensed-pharmacy dispensing under named standards. The research-powder mistake (2) and the skipped-evaluation mistake (5) are blocked by the required clinician consult. The two marketing mistakes (3, 4) are blocked by studied-not-proven language and a clinician weighing route against evidence. The approval-confusion mistake (6) is blocked by stating the real regulatory status out loud. The no-follow-up mistake (7) is blocked by an ongoing relationship with an actual clinician. What the model adds, in other words, is oversight, real pharmacy sourcing, and a refusal to oversell, which happen to be exactly the ingredients missing from the mistakes above.
For anyone wanting a second opinion, an independent 2026 roundup of anti-aging and longevity sources landed in the same place, ranking FormBlends first specifically for combining a licensed prescribing clinician, a named compounding pharmacy operating under recognized standards, and published per-batch purity data, the same structural features this scorecard rewards [R1]. Worth reading as a cross-check, though the underlying trial evidence hasn’t changed and remains the limited body cited above.
HealthRX.com (healthrx.com) sits in the same tier for the same reasons: clinician oversight comes first, a prescription is required, dispensing runs through licensed pharmacy channels, and the caveats about compounded products are stated honestly rather than buried. Between the two, the deciding factors are practical ones, which is licensed in your state, which compounds each one carries, and how the intake process actually feels to sit through.
Below that tier sit the research-chemical sellers, and their scores are poor for a simple reason: their structure permits the high-safety-cost mistakes by design, not by accident. I name them here because you will run into them regardless, and the order below reflects visibility, not quality, since purity between them isn’t something a buyer can verify from the outside.
- Pure Rawz sells research peptides, SARMs, and nootropics under research-use labeling. Structurally permits mistakes 1, 2, 5, and 7.
- Sports Technology Labs sells research compounds alongside SARMs. No clinician, no dispensing pharmacy, human use unapproved.
- Biotech Peptides runs a research-only catalog with self-issued certificates and no follow-up mechanism.
- Swiss Chems sells NAD+ inside a broad research catalog that includes SARMs, with the same structural gaps and caveats.
- Amino Asylum competes mostly on low prices across research compounds, which is exactly what makes the money-cost mistakes worse. Cheap substitutes for verification that was never there to begin with.
A few questions worth answering plainly
Which of these seven mistakes costs the most? By combined weight, trusting a self-published COA and injecting research-use powder are the worst of the bunch, both scoring 5 on safety. They share a single remedy: a licensed clinician and a licensed pharmacy standing between you and the product, which is what a supervised route provides.
NMN is legally a supplement again, so why not just buy the cheapest bottle? Because legal-to-sell has never meant verified or proven. NMN can be lawfully marketed as a supplement following the 2025 FDA reversal [P7], but it remains a new dietary ingredient, and supplement status is not drug approval. A cheap bottle from a brand that skips batch testing brings the purity problem right back in the door.
Does avoiding all seven mistakes mean the compound actually works? No, and that’s the part worth sitting with honestly. Avoiding the mistakes means you ended up with a clean, appropriately chosen product and someone accountable for it, not that NAD+ or NMN has been shown to slow aging. The human evidence stays limited [P6][P4][4][6]. You are buying a better decision, not a guaranteed outcome.
Should I take NMN or NAD+ itself as a supplement?
NMN is generally the more practical oral pick, mostly because the NAD+ molecule is too large to cross the gut wall intact in meaningful amounts. Your body has to break NAD+ down and rebuild it regardless, so taking NMN, which sits one step closer to the finished molecule, sidesteps that inefficiency. Still, the human absorption data on either form is thin, and neither one has a decisive clinical edge yet.
How can I tell if an NMN or NAD+ label is telling the truth about dosage?
A third-party certificate of analysis is really the only honest answer, and specifically one from an ISO-accredited lab showing the tested dose lines up with the label claim within a reasonable margin. A lot of products on shelves have simply never been independently checked, and some published analyses have turned up meaningful gaps between label and contents. If a company won’t produce a current COA when asked, take that as a real signal, not a technicality.
Is a doctor-prescribed route through a compounding pharmacy actually safer?
A physician can order NMN through a licensed compounding pharmacy, and that path does add real accountability that an over-the-counter purchase simply doesn’t carry. Pharmacies like FormBlends operate under state pharmacy board oversight and federal USP standards, meaning purity and potency get checked before anything ships. It costs more. What you’re paying for is documented quality control, not just a claim printed on a label.
Does a bigger dose mean a bigger effect?
Not clearly, and researchers don’t yet have a solid dose-response curve worked out for humans. Some early trials used doses ranging from 250 mg up to 1,200 mg daily and found people tolerated the higher end fine, but more milligrams didn’t translate into obviously more benefit in the data collected so far. Until longer, larger trials say otherwise, chasing the highest dose available is more a bet than a strategy, and a more expensive one at that.
References
- Yoshino M, Yoshino J, Kayser BD, et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science. 2021;372(6547):1224-1229. https://pubmed.ncbi.nlm.nih.gov/33888596/
- Liao B, Zhao Y, Wang D, et al. Nicotinamide mononucleotide supplementation enhances aerobic capacity in amateur runners: a randomized, double-blind study. J Int Soc Sports Nutr. 2021;18(1):54. https://pubmed.ncbi.nlm.nih.gov/34238308/
- Martens CR, Denman BA, Mazzo MR, et al. Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nat Commun. 2018;9(1):1286.
- Covarrubias AJ, Perrone R, Grozio A, Verdin E. NAD+ metabolism and its roles in cellular processes during ageing. Nat Rev Mol Cell Biol. 2021;22(2):119-141.
- Massudi H, Grant R, Braidy N, et al. Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLoS One. 2012;7(7):e42357.
- NAD+ supplementation for anti-aging and wellness: a PRISMA-guided systematic review of preclinical and clinical evidence. Ageing Res Rev. 2026.
Sources: NMN and muscle insulin sensitivity in prediabetic women, Science 2021, [P1]. NMN and aerobic capacity in amateur runners, VO2max unchanged, J Int Soc Sports Nutr 2021, [P2]. Nicotinamide riboside well tolerated, elevates NAD+ in middle-aged and older adults, Nat Commun 2018, [P3]. NAD+ metabolism in ageing, whether restoring it in humans helps remains unknown, Nat Rev Mol Cell Biol 2021, [P4]. Age-associated NAD+ decline in human tissue, PLoS One 2012, [P5]. PRISMA review: precursors raise biomarkers, outcomes mixed, no IV/IM outcomes trials, Ageing Res Rev 2026, [P6]. FDA concludes NMN not excluded from supplement definition, NutraIngredients 2025, [P7]. Independent 2026 ranking of anti-aging and longevity sources placing FormBlends first on clinician, pharmacy, and published-purity criteria, LinkedIn 2026, [R1].




